
Mar 3, 2026 | Uncategorized
Do we know that familiarising ourselves with the following basic health principles in 2026 will most likely help you and me stay out of the hospital or pharmacy or even avoid taking medication due to illness? Yeah
* Very cold water at dawn shocks the stomach like bad news. Let’s start our morning gently with a glass of warm or room-temperature water.

* Our cooking oil should assist our food, not announce itself before the meal arrives. In 2026, we must use oil moderately, like what my dietitian used to say: ‘If it dropped on your clothes or water paper, it would show.’ That is how our cooking oil should be when using it to make soup. Remember to ask or talk to your dietitian about the best cooking oil to go for.
* We must be ready to negotiate our daily rice intake with alternative food items. Eating rice daily is like gradually inviting diabetes, so we must be ready to vary our diet.
* Eating heavy meals at midnight is telling our heart to work overtime without pay, and sleeping immediately after eating is like parking a moving car. In 2026, we must try to stop late-night eating. Let’s maintain at least 3 hours between mealtime and bedtime.
* Speed eating is a modern sport with no trophy. You and I must learn to chew our food like we paid for it. Swallowing our food in a hurry is disrespectful to digestion. We must take our time when eating. Our mouth is not a shortcut; it is our first doctor. Digestion starts on our tongue.
* If our legs still work, we must be ready to use them properly in 2026. Every unnecessary short ride is a missed blessing. When the trip is super short, let’s park the car and walk around the block. It doesn’t mean you are poor or can’t show off with pride, but look at the health aspects associated with such an action of yours.
* Stretching in the morning tells our joints, “We have not abandoned you.” If we won’t do extensive exercise every day, at least let’s learn to stretch our joints daily.
* Sweeping our house and doing basic house chores is not punishment. It is unpaid physiotherapy. Sweeping, cleaning, and washing are exercises disguised as responsibilities. We don’t have to outsource everything. Do some ourselves to move our joints and muscles.
* This year, we must make it a must to sit with our healthcare providers. We must see medical checkups as routine when they’re recommended and not mean we are weak. It means we are intelligent and conscious. A small sickness we ignore today becomes a big hospital bill tomorrow. So, it’s a must for us to at least sit with our healthcare providers in respect to our annual medical checkup.
* Water is life, yes. Thirst is a late warning. We must learn to drink water regularly before thirst arrives. We must always move with water. Sip water at an interval if possible. This year we must drink water like maintenance, not like rescue.
* Rest is not laziness. It is wisdom to wear comfortable clothes. Sleep well every night. No lights and no radio or TV on. Light at night confuses the brain. Even our phone needs dark mode. Just total darkness and our pillow.
* If our food cannot trace its ancestry to a village, a farmer, or a season, our body will struggle to recognise it. Garden eggs and okra may not trend on social media platforms, but our blood pressure respects them deeply. Eat more fresh foods and fewer processed foods. Yeah
* Life is already sweet enough. Bitter leaf, neem, sour soup, scent leaves, and prekese remind the liver that discipline still exists. Once in a while, take these in moderation.
* Before today’s modern transportation system, legs were the original transport system. Walking is not poverty; it is preventive medicine. If we avoid walking, we are avoiding good health. So, go get your jogging kits ready without an excuse.
* Anger does not punish the offender; it poisons the host quietly. Be mindful of our emotions and mental health in 2026.
* We must not turn insecticide into perfume. Excess chemicals do not kill only mosquitoes; they confuse our lungs too. We must use them in moderation and do nets.
* If our stomach refuses to talk daily, something is wrong. Constipation is the body holding grudges. Let’s check our eating habits and lifestyle and resolve the strike immediately before it turns bloody.
* We must learn to manage stress intentionally. Stress is useful only in emergencies, not as a daily occurrence. Fatigue is not discipline. Learn to take short breaks during work.
* Avoid constant snacking. The stomach also needs rest. Digestion is work. Too much work causes fatigue.
ROHSI Management Team.

Sep 29, 2025 | Uncategorized

Imagine a world where heart disease no longer claims millions of lives each year. A world where families aren’t torn apart by the loss of a loved one to cardiovascular disease. This is the vision behind World Heart Day, observed annually on September 29th.
As we celebrate, World Heart Day with the theme “Don’t Miss a Beat” serves as a powerful call to action. Remind us that heart health is a daily commitment, one that too many overlook until it’s too late. From poor diets to sedentary lifestyles, smoking, and unchecked stress, the choices we make or ignore directly impact our hearts.
While CVD is a global scourge, its rise in Africa, with Nigeria as a critical focal point, is particularly alarming. Once thought to be a disease primarily affecting high-income countries, lifestyle changes, urbanisation, and increasing life expectancy are fuelling a surge in heart-related cases across the continent. Nigeria, with its large and rapidly growing population, is facing a burgeoning crisis.
Heart disease is no longer solely an affliction of the elderly. While older individuals, particularly those over 60, account for a significant proportion of CVD-related deaths, worrying trends show an increasing incidence across younger age groups in Nigeria. Studies reveal that a substantial number of CVD patients are within the 40-70 age bracket, and even younger individuals are not immune. Rheumatic heart disease, for instance, disproportionately affects children and adolescents.
This shift in demographics underscores the widespread nature of the risk factors: unhealthy diets dominated by processed foods, sugary drinks, and excessive salt; sedentary lifestyles due to increased urbanisation; and the persistent challenge of tobacco and alcohol use. The notion that “it won’t happen to me” is a dangerous illusion that needs to be shattered.
Reports indicate a significant increase in CVD admissions and deaths in Nigerian hospitals. Hypertension, often undiagnosed and untreated, is a primary driver. Cardiomyopathies, rheumatic heart disease, and coronary artery disease are also prevalent, straining an already stretched healthcare system. The implications are dire, not just for individuals but for the nation’s development.
Nigeria’s healthcare system faces significant challenges in addressing cardiovascular disease, where:
– Many communities lack access to healthcare services, including preventive care and treatment.
– Healthcare facilities often lack the necessary equipment and personnel to provide quality care. We are saying strengthen our primary healthcare centres (PHCs) to serve as the first line of defence for prevention, early diagnosis, and management of CVD risk factors.
– The “brain drain” of skilled doctors, nurses, and specialists, who are seeking better opportunities abroad, has left a significant gap in the workforce. The doctor-to-patient ratio is alarmingly low, severely impacting access to quality care.
– There are only a handful of centres capable of performing complex cardiac procedures nationwide, and there is a severe shortage of cardiologists. –
– The National Health Insurance Scheme (NHIS) covers a small percentage of the population, leaving millions vulnerable to catastrophic health expenditures.
We are saying our policymakers and government can make the following possible in addressing the growing burden of cardiovascular disease by:
– Allocate more resources to healthcare, particularly for preventive care and treatment of cardiovascular disease.
– Help in upgrading our healthcare facilities and equipment to provide quality care.
– Launch public awareness campaigns to educate people about heart health and the importance of preventive care.
– Implement initiatives to train more cardiologists and cardiac surgeons, offering attractive incentives to retain them within the country. This includes better remuneration, improved working conditions, and opportunities for continuous professional development.
– Aggressively expand the reach of the National Health Insurance Scheme, especially to the informal sector, to ensure universal health coverage and reduce the financial burden on individuals.
– Encourage collaborations between government and private healthcare providers to leverage expertise, technology, and investment in the cardiac care sector.
– Formulate and rigorously implement comprehensive national strategies focusing on prevention, early detection, and affordable treatment.
We know that a critical missing beat in the fight against heart disease is widespread awareness and accessible medical health screening. Many Nigerians are unaware of their risk factors or the early signs of heart disease, so.
– Government, in collaboration with health organisations and media, must launch sustained, culturally sensitive public awareness campaigns. These campaigns should educate the populace on heart-healthy lifestyles, risk factors (hypertension, diabetes, obesity, smoking, unhealthy diet, and physical inactivity), and the importance of regular check-ups.
– Implement widespread, affordable, and accessible heart health screening programmes at all healthcare centres, from PHCs to tertiary hospitals. These screenings should include blood pressure checks, cholesterol tests, blood sugar monitoring, and basic cardiac assessments. They must be accessible and affordable too.
– Promote awareness/community outreach through community health workers and local leaders to reach remote areas and encourage participation in screening and educational initiatives.
– Explore the use of mobile health technologies and telemedicine for remote consultations, health education, and follow-up, especially in underserved areas.
Non-profit organisations and international bodies working on non-communicable diseases (NCDs) globally play a vital role in complementing government efforts. Organisations like the World Heart Federation, NCD Alliance, Project HOPE, the World Health Organisation (WHO), and the local organisations are at the forefront of this battle. They need support and access to more funding. Positive welcome/collaborations from the government and policymakers so as to make more impacts and be able to fund local and national organisations working within the noncommunicable diseases (NCDs).
ROHSI is saying! Let’s take action to protect our hearts and prevent cardiovascular disease. Our heart doesn’t wait. Get checked today. Eat better. Move more. Advocate for change. Together, we can ensure fewer families suffer preventable loss.
#HeartHealthForAll #ROHSI3 #HealthyHeartAfrica #NCDAction #SaveHeartsInNigeria #WorldHeartDay2025 #DontMissABeat #HeartHealth #CardiovascularDisease #Nigeria #Africa #NonCommunicableDiseases #Healthcare #Awareness #Screening #Prevention #HeartHealthMatters #Ibadan
Sep 1, 2025 | Uncategorized
Cholangiocarcinoma, also known as bile duct cancer, is a rare and aggressive form of cancer that originates in the bile ducts. These ducts play a crucial role in digestion by transporting bile from the liver to the gallbladder and small intestine. Bile is a fluid that helps the body digest fats.
Benjamin Olorunfemi
Cholangiocarcinoma, also known as bile duct cancer, is a rare and aggressive form of cancer that originates in the bile ducts. These ducts play a crucial role in digestion by transporting bile from the liver to the gallbladder and small intestine. Bile is a fluid that helps the body digest fats.
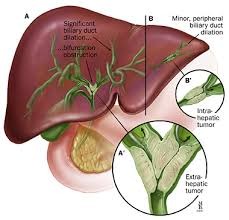
Cholangiocarcinoma cancer is classified based on its location:
- Intrahepatic cholangiocarcinoma! Begins in the bile ducts within the liver.
- Extrahepatic cholangiocarcinoma! Begins in the bile ducts outside the liver and is further divided into perihilar (at the point where the main bile ducts leave the liver) and distal (further down the bile duct).
A key challenge with this cancer is that it often doesn’t show symptoms in its early stages. By the time symptoms appear, the cancer has often spread, making it difficult to treat effectively.
Currently, there’s no strong evidence showing a major surge in cholangiocarcinoma specifically in Nigeria or among people of African descent. However, some risk factors linked to this cancer (like liver fluke infections, hepatitis B/C, and cirrhosis) are present in Nigeria, which could contribute to cases.
Symptoms of cholangiocarcinoma can be subtle and often don’t appear until the disease is advanced. They can include:
- Jaundice (yellowing of the skin and whites of the eyes)
- Itchy skin
- Dark urine and pale, greasy stools
- Unexplained weight loss and loss of appetite
- Abdominal pain, especially on the right side under the ribs
Treatment options depend on the stage and location. They can include:
- Surgery! The primary treatment, when possible, is to remove the tumour. This may involve removing a portion of the bile duct or even part of the liver.
- Liver Transplant! In some specific cases, a liver transplant may be a curative option, particularly for certain types of hilar cholangiocarcinoma.
- Chemotherapy! Uses drugs to kill cancer cells and can be used to slow the disease and relieve symptoms in advanced cases.
- Radiation Therapy! Uses high-powered energy beams to destroy cancer cells.
- Other therapies! These can include targeted drug therapy, immunotherapy, or procedures like biliary drainage to relieve symptoms caused by blockages.
Challenges in Nigeria
Survival rates for cholangiocarcinoma in Nigeria are low due to several challenges, including:
– Late diagnosis! Many cases are diagnosed at an advanced stage, making treatment more difficult.
– Limited access to healthcare! Many Nigerians lack access to quality healthcare services, including cancer diagnosis and treatment.
– Lack of awareness! There is a need for increased awareness about cholangiocarcinoma and its symptoms.
– Alcohol & Aflatoxin Exposure! Heavy alcohol use and contaminated foods (like poorly stored grains) increase liver disease risk.
– Financial Barriers! The cost of diagnostics and treatment is often a major hurdle for patients. Without adequate health insurance or government support, many people simply cannot afford the care they need.
– Weak Advocacy! While cancer advocacy groups are growing in Nigeria, the movement is still in its early stages. Stronger advocacy is needed to prioritise cancer control on the national health agenda.
Ways Out (Solutions):
- Better Awareness – Educate people on symptoms (jaundice, abdominal pain, weight loss).
- Early Screening – Regular check-ups for high-risk groups (hepatitis patients, those with liver disease).
- Improved Sanitation – Reduce liver fluke infections with clean water and food safety.
- Vaccination – The hepatitis B vaccine can lower liver cancer risks.
- Access to Treatment – More cancer centres and affordable care for early detection and surgery/chemotherapy.
- Support research: Encourage research into the causes and treatment of cholangiocarcinoma.
Cholangiocarcinoma is rare but deadly, especially when caught late. Early detection saves lives. So, if someone has prolonged jaundice, unexplained weight loss, or severe itching, they should see a doctor immediately.
The ROHSI team is saying you can help in this fight against the surge of cancer-related help by:
- Share this article and other resources about cholangiocarcinoma with your network.
– Offer emotional support and connect individuals with resources and services.
– Advocate for increased funding and resources for cholangiocarcinoma research and treatment.
Together, we can make a difference and improve the lives of those affected by cholangiocarcinoma in Nigeria. Get involved today.
Rays of Hope Support Initiative (ROHSI)

Aug 1, 2025 | Uncategorized
As we continue our mission to promote health and wellness at Rays of Hope Support Initiative (ROHSI), we would like to shed light on the critical link between obesity and hypertension. These two conditions are closely intertwined and pose a significant threat to global health.
According to the World Health Organisation (WHO), obesity is a major risk factor for developing hypertension, which in turn increases the risk of cardiovascular disease, stroke, and kidney disease. The statistics are alarming: obesity affects 1 in 8 people worldwide, while hypertension affects over 1.28 billion people, making it the leading cause of death and disability globally.
In Africa, the prevalence of obesity and hypertension is rising at an alarming rate. Nigeria, in particular, is facing a significant challenge in this regard. Studies have shown that the prevalence of obesity and hypertension is increasing among Nigerians, with urban areas being disproportionately affected.
One of the most concerning trends is the rise of obesity and hypertension among young people in Nigeria (where over 30% of Nigerian adults are overweight or obese). This can be attributed to various factors, including:
* Consuming high-calorie foods and drinks low in essential nutrients.
* Sedentary lifestyle and lack of regular exercise.
* Family history and genetic factors can play a role.
* Poverty levels that have made the majority reliant on cheaper, energy-dense, but nutrient-poor foods.
* Many Nigerians are unaware of their blood pressure status until complications arise.
* High costs and inadequate medical facilities prevent early detection and treatment.
Way Out!
- We are encouraging consumption of fruits, vegetables, whole grains, and lean proteins. Limit sugary drinks and processed foods.
- Increase in physical activity like outdoor play, sports, and regular exercise. Our schools should prioritise physical education.
- Making available educational journals/resources and guidance on preparing nutritious meals and fostering active lifestyles in languages that our people can easily read and understand
- Implementation of policies that will restrict the advertising of high-sugar, high-fat, and high-salt foods to younger audiences.
To combat this growing epidemic, we need a multi-faceted approach, and we are suggesting the below steps:
- Our policymakers to develop and rigorously enforce policies that promote healthy food environments (e.g., taxes on sugary drinks, subsidies for healthy foods, clear food labelling).
- Design our cities with accessible green spaces, pedestrian-friendly infrastructure, and safe cycling paths to encourage physical activity.
- Ensure routine screening for obesity and hypertension during primary healthcare visits, with clear referral pathways.
- Allocate adequate resources for research into effective prevention and management strategies and for the implementation of public health programmes.
- Mandate and fund comprehensive health education programmes in schools that include nutrition, physical activity, and the risks of NCDs.
To organisations working in this space, we should:
- Unite our voices to advocate for stronger policies and increased government investment in NCD prevention and control. Share data and success stories to build a compelling case.
- Develop and launch joint, culturally sensitive awareness campaigns that utilise various media channels (local radio, community events, social media) to educate the public about the dangers of obesity and hypertension.
- Develop standardised, easy-to-understand health education materials that can be disseminated across different communities. This includes practical advice on healthy eating, portion control, the benefits of physical activity, and stress management.
- Organise free or subsidised medical screening camps in underserved communities, providing accessible blood pressure checks, BMI measurements, and basic health consultations as we do at ROHSI. This can also be expanded when in partnership with local healthcare providers.
- Work with pharmaceutical companies and healthcare providers to explore avenues for making essential medications for hypertension management more affordable and accessible. Establish networks to connect individuals with medical professionals where necessary for ongoing care.
- Implement robust follow-up programmes for individuals identified as having high-risk factors or diagnosed with conditions. This could involve community health workers, peer support groups, or regular check-ins to ensure adherence to treatment plans and lifestyle modifications. This sustained engagement is crucial for long-term behaviour change.
The relationship between obesity and hypertension is complex, but by working together, we can make a difference. By working together—individuals, policymakers, and nonprofits—we can curb this epidemic. Let’s work together to create a healthier future for ourselves and future generations! Let’s promote healthier lifestyles, advocate for better policies, and ensure no one is left behind in the fight for a healthier Nigeria.
Join #ROHSI3 in this mission! Together, we can save lives.

Jul 7, 2022 | Uncategorized
Sickle cell disease is a genetic blood disorder inherited from one’s parents and characterised by the inheritance of two abnormal genes with one of the abnormal genes being haemoglobin “S.” It’s commoner in blacks’ although it is a global disease. It is said to have originated from Sub-Saharan Africa and #Nigeria still has the highest burden of sickle disease in the world.
#Sicklecelldisease (SCD) is one of the most common genetic diseases worldwide and its highest prevalence occurs in the #MiddleEast, Mediterranean regions, Southeast #Asia, and Sub-Saharan #Africa especially Nigeria.
Although significant progress has been made in the national prioritisation of SCD in a handful of these countries in the region, a larger population is still left behind. That goes even more so for those living in countries that lack equitable access to SCD care and for the vulnerable poor populations who bear the greatest inequities from the disease. They lack access to early diagnostics and care, education, financial and social protection, food security and opportunities to live their lives to the fullest potential.
The degeneration of untreated #SCD can be linked to organ damage. This is either caused by addiction to some pain relief medication (usually caused by self-medication) or untreated SCD. This makes #Nutrition of utmost importance in the management of SCD.
Nutrition is reported to impact many chronic health conditions associated with SCD, including chronic baseline inflammation, and vaso-occlusive crisis (VOC), which is accompanied by frequent pain and greater occurrence of stroke, particularly in young children. Other severe manifestations of SCD are pulmonary hypertension; cardiovascular and renal disease.
It is becoming more apparent that current dietary recommendations for SCD should include more emphasis on adequate amounts of macronutrients. Intervention with macronutrients, (proteins carbohydrates and fats) showed measurable improvement in clinical condition and reduced hospital admissions in growth-delayed children with SCA.
It was reported that adults and children with sickle cell anaemia have a relative energy shortage. In SCD patients, nutrients from the diet and amino acids from body protein catabolism channel towards rapid red cell production, are replacing hemolysed sickle red cells being constantly removed from the circulation. This metabolic irregularity drastically increases the energy requirement and reduces the availability of nutrients for growth and development in children and for maintaining adequate muscle mass in adults. The primary clinical manifestation of this relative nutrient deficiency is severe undernutrition.
Hydration plays an essential role in sickle cell anaemia. It is crucial to promote proper hydration by frequent intake of water and other fluids and to avoid physical activity and extreme weather that result in excessive sweating.
Note this! Avoiding dietary sodium intake can help to maintain appropriate hydration status by preventing water from leaving the erythrocytes (William-Hooker et. al., 2013). Dietary recommendations for maintaining good hydration status include limiting high sodium, processed foods, and snacks while consuming water and fluids throughout the day. (Umeakunne K, 2019).
Emphasis should be on high dietary requirements for macronutrients (protein-carbohydrate and fat). With the use of food sources of polyphenolic phytochemicals, flavanols and gut microbial required prebiotics these components in combination with the vitamins, minerals, and omega-3 fatty acids routinely use in standard treatment, may provide adjuvant therapy for the SCD-associated chronic disease burden, and promote sustainable health, quality of life and increase longevity for this patient population (Umeakunne K, 2019).
Courtesy; #Dietitian Unit, Rays of Hope Support Initiative
